
Bariatric surgery complications:
- Are almost never life-threatening (99.9% survival rate)
- Are non-existent for about 93% of patients (30-day complication rate is 7%)
- Risk can be further minimized in a number of ways
- Differ depending on which procedure you choose
Read the sections below for everything you need to know about weight loss surgery complications.
TABLE OF CONTENTS
Click on any of the topics below to jump directly to that section
- Obesity Risks Vs Surgery Risks
- How to Reduce Risk
- Complications By Procedure
- List & Definitions
- Patient Community & Expert Advice
SECTION SUMMARY:
- Read about the possible complications of gastric sleeve, gastric bypass, the Lap-Band, Duodenal Switch, AspireAssist, & the gastric balloon below
Complications and side effects are more common and more pronounced among the more-involved, higher-weight-loss procedures:
- Gastric sleeve
- Gastric bypass
- Lap-Band
- Duodenal switch
They can be especially pronounced for the two procedures that rearrange your digestive system (they also lead to the most long-term weight loss):
- Gastric bypass
- Duodenal switch
Complications and side effects are less common and less pronounced among the less-involved, lower-weight-loss procedures:
- Gastric balloon
- AspireAssist
To simplify: the more weight loss a procedure results in, the higher the risk of complications and side effects.
Tap here to expand list of complications by procedure.
| Issue | Gastric Sleeve | Gastric Bypass | Gastric Balloon | Lap-Band | Duodenal Switch | AspireAssist |
|---|---|---|---|---|---|---|
| Abscess | – | – | ||||
| Band Problems (band erosion, band infection, band intolerance, band leak, band slippage) | – | – | – | – | ||
| Blood Clots | – | – | ||||
| Bowel Obstruction | – | – | ||||
| Deep Vein Thrombosis | – | – | ||||
| Evisceration & Incisional Hernia | – | – | ||||
| Gastric Fistula | – | – | ||||
| Gastrointestinal Leaks | – | – | – | |||
| General Anesthesia Complications | – | – | ||||
| Heart Attack | – | – | ||||
| Hemorrhage (Bleeding) | – | – | ||||
| Hiatal Hernia | – | – | ||||
| Hypoglycemia | – | – | – | – | – | |
| Infection | – | |||||
| Organ Injury During Surgery | – | |||||
| Peritonitis | – | – | – | |||
| Pneumonia | ||||||
| Port Problems (port flip/inversion or dislodgement, port leak, port infection, port dislocation) | – | – | ||||
| Port Problems (port flip/inversion or dislodgement, port leak, port infection, port dislocation) | – | – | – | – | – | |
| Pouch Dilation | – | – | – | – | – | |
| Pulmonary Embolism | – | – | ||||
| Respiratory Failure | – | – | ||||
| Stenosis/Stricture | – | – | – | |||
| Stoma Obstruction | – | – | – | |||
| Stroke | – | – | ||||
| Thrombophlebitis | – | – | ||||
| Wound Reopening | – | – | ||||
| Wound Sepsis | – | – |
Tap here to expand list of side effects by procedure.
| Issue | Gastric Sleeve | Gastric Bypass | Gastric Balloon | Lap-Band | Duodenal Switch | AspireAssist |
|---|---|---|---|---|---|---|
| Abdominal Discomfort | – | – | – | – | – | |
| Anemia | – | – | – | |||
| Body Aches | – | – | ||||
| Body Feeling Changes | – | |||||
| Bowel Function Changes (diarrhea, constipation, foul-smelling bowel movements and flatulence, difficulty swallowing, gurgling noises) | — | |||||
| Dehydration | – | – | ||||
| Dental Problems | – | – | – | – | – | |
| Dumping Syndrome | – | – | – | – | – | |
| Dyspepsia (Indigestion) | – | – | ||||
| Esophageal Dilation | – | – | ||||
| Esophagitis | – | – | ||||
| Food Trapping | – | – | – | – | – | |
| Gallstones | – | – | ||||
| Gastritis | – | – | ||||
| Gastroesophageal Reflux Disease (GERD) | – | – | ||||
| Hair Loss | – | – | ||||
| Intolerance to Certain Foods | – | |||||
| Kidney Stones | – | – | – | – | ||
| Marginal Ulcers | – | |||||
| Nausea, Vomiting and/or Stomach Cramps | ||||||
| Skin Changes (e.g. acne, dry skin, sagging skin, etc.) | – | – | ||||
| Thrush (Yeast Infection) | – | – | ||||
| Vitamin & Mineral Deficiency / Malnutrition / Malabsorption | – | – | ||||
| Weight Regain | – |
For more information about complications and side effects by weight loss procedure, click the links below:
SECTION SUMMARY:
- A to Z list of complications and definitions
Click on a letter below to jump to a bariatric surgery complication beginning with that letter or scroll down the page to review the complete list of complications, definitions (10), and treatments:
| A | B | C | D | E | F | G | H | I | J | K | L | M | N | O | P | Q | R | S | T | U | V | WXYZ |
Abdominal hernias – a protrusion of an organ or part through connective tissue or through a wall of the cavity in which it is normally enclosed – also called a “rupture”. Most hernias are treated with surgery unless another condition makes surgery inadvisable.
Abscesses – a localized collection of pus surrounded by inflamed tissue. Abscesses are drained percutaneously (through the skin) or through surgery.
Aches – see Body Aches.
Alcohol Use Disorder (AUD) – a physical and emotional dependence on alcohol that leads to the inability to cease drinking, even after serious lifestyle, health, or legal issues.
Anastomotic Leaks happen when the surgical connection made during bariatric surgery leaks digestive contents into the abdomen. See Gastrointestinal Leaks for more.
Anesthesia complications – See General Anesthesia Complications.
Anemia – a condition in which the blood is deficient in red blood cells, in hemoglobin or in total volume. Anemia is a common issue stemming from vitamin deficiency after malabsorptive bariatric surgery procedures.
Anemia following bariatric surgery is routinely treated with iron orally and, when indicated, with intravenous iron infusions; blood transfusions are rarely required. Finding and treating anemia before surgery with iron and ESA therapy has been found to be effective at both avoiding transfusions and reducing surgery risks (11).
- Band Erosion (also called “Band Migration “) – occurs in gastric banding (lap band surgery) and vertical banded gastroplasty patients as these are the only bariatric procedures involving a band. Band erosion occurs when the band actually grows into the stomach. The only treatment is a permanent removal of the band. See our Lap Band Erosion page for more information.
- Band Intolerance– when patients do not respond well (i.e. excessive and continued vomiting) to the band placed during vertical banded gastroplasty or gastric banding (lap band) surgery. Will probably require that the band be permanently removed.
- Band leak (1.1% – 4.9% of lap band patients) – patients can usually tell if their lap band system has a leak if their feelings of restriction (how much they can eat) decrease over time without the doctor unfilling the port. To determine if you have a lap band leak, your doctor may inject colored fluid and take an X-Ray to see if any of the colored fluid is present (from a leak) outside of the lap band system. Surgery is usually required to repair it.
- Band Migration – See Band Erosion.
- Band Slippage – occurs when the lower part of the stomach “slips” up through the band, creating a bigger pouch above the band (only occurs after gastric lap band surgery and vertical banded gastroplasty as these are the only bariatric procedures involving a band). As many as 1 in 10 patients experience this with gastric banding (lap band surgery), and either removing fluid from the lap band or surgery is required to repair it. Symptoms include vomiting and reflux. It is diagnosed by drinking a dye and using X-Ray to observe it. For information about surgical techniques to reduce the risk of slippage, see our Gastric Lap Band Procedure page.
Bleeding – See Hemorrhage.
Blood Clots (also called “thrombus”) – overweight people have a higher risk of developing blood clots during and after any kind of surgery. Blood thinners are usually administered during and after surgery to avoid them, along with special devices that squeeze the lower legs to keep the blood flowing. Walking around periodically after surgery is also very effective. Symptoms of blood clots include swelling or pain in the legs and can be diagnosed by your doctor with an ultrasound. If clots occur, they are treated by a taking a prescribed blood thinner. If left untreated, clots can lead to a pulmonary embolism. Prior to surgery, be sure to tell your doctor whether you or anyone in your family has a history of clotting. Smoking will increase your risk, so if you are a smoker it is recommended that you stop smoking as soon as possible before surgery – no later than two months out. For more information, see our Blood Clot Symptoms, Treatments & Prevention page.
Body Aches – should pass with time. If they become unbearable, talk with your doctor about which pain relievers are safe. You should typically avoid NSAIDs (non-steroidal anti-inflammatory drugs) such as ibuprofen or Aleve.
- Feeling cold – this is caused by both your changed metabolism and weight loss and the fact that you have less fat insulating your body.
- Weak or tired feeling – should pass with time, especially once your new bariatric diet is in place and, as soon as you are feeling up to it, your weight loss surgery exercise program has begun.
Bowel Function Changes (especially more frequent bowel movements and/or foul-smelling flatulence) – bowel function after bariatric surgery may change in a number of ways, (12) including…
- Diarrhea or loose stools (especially after gastric sleeve surgery, duodenal switch, gastric bypass surgery, and mini gastric bypass surgery) – usually completely dependent on diet – you will need to figure out and avoid foods that “trigger ” diarrhea. Could also be the result of lactose intolerance which would require dairy products to be removed from your bariatric diet.
- Constipation (especially after gastric banding (lap band surgery), gastric bypass, mini gastric bypass, and rarely after duodenal switch) – usually fixed by increasing the amount of water you are drinking and taking fiber supplements such as Fiber-Stat’s liquid fiber supplement.
- Foul-smelling bowel movements & flatulence (especially after duodenal switch) – as with diarrhea, it is usually dependent upon diet.
- Difficulty swallowing (“dysphagia”) (after all restrictive procedures) – caused by eating too quickly, too much or not chewing food enough and can usually be fixed by avoiding these issues. (See our Bariatric Eating page to learn about proper eating techniques that will avoid problems.)
- Gurgling Noises – not necessarily uncomfortable or dangerous, but it’s worth noting. Gurgling noises are completely normal and are due to air in the stomach and the different way that your new digestive system pushes the air through. The best way to avoid gurgling noises is to avoid swallowing air (i.e. avoid carbonated beverages, sipping through a straw, eating or drinking too quickly and chewing gum).
Bowel Obstruction – also called an “internal hernia”, is a lifelong risk following bariatric surgery that occurs when the intestines twist and prevent the flow of food and digestive fluids. Patients with this condition usually experience abdominal pain, abdominal swelling, or vomiting. A doctor will confirm the diagnosis with a CAT scan or through surgery, and surgery may or may not be needed to treat it.
Bowel obstructions post-surgery are more commonly associated with adhesions and not internal hernias, although both are known to be associated with post-op bowel obstructions.
Bowel Perforation – See Organ Injury During Surgery.
Cold feeling – See Body Feeling Changes.
Candy Cane Syndrome – A possible complication after gastric bypass, candy cane syndrome happens when a no-longer-functioning part of the small intestine near the new junction of the stomach and small intestine begins to cause abdominal pain, nausea, and vomiting. The “Candy Cane” (the non-functioning portion of the intestine) will need to be laparoscopically removed, but once the “candy cane” is gone, 94% of patients experience complete resolution of their symptoms (REF).
Death – the bariatric surgery mortality rate is extremely low at about 0.135% and has continued to drop over time (13). For a boiled down list of issues that directly contribute to mortality risk, see our Bariatric Surgery Risks page.
Deep vein thrombosis (DVT) is a risk after any surgery (bariatric or otherwise) marked by the formation of a thrombus within a deep vein (as of the leg or pelvis) that may be asymptomatic or accompanied by symptoms (such as swelling and pain). DVT is potentially life-threatening if dislodgement of the thrombus results in pulmonary embolism. Preventive measures are extremely important, especially for those with a history of blood clotting problems. Blood thinners and compression stockings help to reduce the risks. Also see Blood Clots.
Dehydration – an abnormal depletion of body fluids. You will need to drink a significant amount of water in the months following surgery – as much as 2 liters per day. Not doing so can lead to nausea and vomiting which can cause even worse dehydration and other problems. In severe cases of dehydration patients must return to the hospital for IV fluids and vitamins.
Dyspepsia (also called indigestion) – inability to digest or difficulty in digesting food; incomplete or imperfect digestion of food; a case or attack of indigestion marked especially by a burning sensation or discomfort in the upper abdomen. Treatment is usually as simple as changing your diet, such as avoiding greasy foods or only drinking liquids for a certain period of time. Alcohol, aspirin, and other drugs are also causes. If diet changes don’t work, antacids and H2 blockers are sometimes prescribed.
Dysphagia (difficulty swallowing) – See Bowel Function Changes.
Dumping syndrome – we have an entire page dedicated to this topic, but in general it’s a condition characterized by weakness, dizziness, flushing and warmth, nausea and palpitation immediately or shortly after eating. It is produced by abnormally rapid emptying of the stomach especially in individuals who have had part of the stomach removed. See our Dumping Syndrome page for more.
Embolism – See Pulmonary Embolism.
Esophagitis -occurring in less than 1% of patients, esophagitis is the inflammation of the esophagus. It is usually treated non-surgically by making the patient comfortable through a change in diet (avoiding fats and chocolate) and/or avoiding/prescribing certain drugs.
Esophageal dilation – is the enlarging of the esophagus (the opening,not necessarily inflammation) and is usually the result of a restrictive procedure. Most cases can be handled through deflation of the band under radiological control (14). GERDsymptoms and vomiting are more frequent in patients who develop esophageal dilation (15).
Evisceration & Incisional hernia – occur when an internal organ or body part protrudes through a surgical incision. More likely to occur with open procedures than with laparoscopic procedures and usually occurs months after surgery. These are typically repaired with surgery.
Fistulas – see Gastric Fistula.
Food trapping – when food gets caught in one of the small openings in your digestive system. Seen in 1 to 2% of lap band patients and treated by deflating the band entirely until the food passes through (16) (17).
Gallstones – small stones of cholesterol formed in the gall bladder or bile passages. Gallstones can be created following rapid weight loss which leads to their development in as many as 1/3 of bariatric surgery patients. As a result, your surgeon may remove your gallbladder during surgery or prescribe bile salt supplements after surgery.
Gastric fistula – occurring in up to 4% of bariatric surgery patients, a gastric fistula is an abnormal passage that leads from an abscess or hollow organ or part to the body surface or from one hollow organ or part to another (18). Sepsis can follow, and surgery is usually required to fix it.
Gastric fistulas are associated with the stomach (i.e. ‘gastric’). However, not all fistulas are associated with the stomach, and other types can occur (such as from an intestine to intestine anastomosis.)
Related risk/complication of gastric fistula: Wound Sepsis
Gastritis – inflammation, especially of the mucous membrane of the stomach. Symptoms include bloating, excessive belching, a burning sensation in the stomach, loss of appetite, nausea, and vomiting. Eating better may get rid of the problem, or your doctor may prescribe antacids or other over the counter medications.
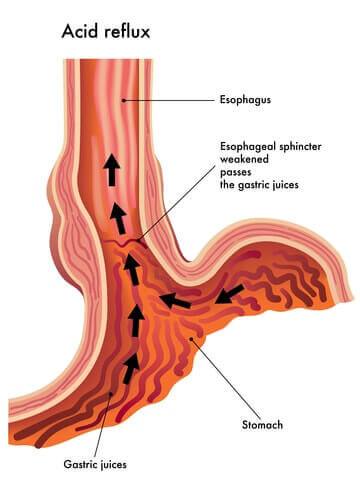
Gastroesophageal reflux disease (GERD) – a highly variable chronic condition that is characterized by periodic episodes of gastroesophageal reflux and usually accompanied by heartburn. It may result in histopathologic changes (change in the microscopic structure) in the esophagus. It also often leads to esophagitis. GERD increases the risk of some bariatric surgery complications such as dumping syndrome and sepsis, but the condition is also improved for many following bariatric surgery (19) (20). Several at-home treatments are effective, including avoiding certain foods and drinks (alcohol, citrus juice, tomato-based food, and chocolate), waiting 3 hours before lying down after a meal, eating smaller meals and elevating your head 8 inches when you lay down. If these don’t work, your doctor may recommend/prescribe antacids, H2 blockers or even Proton Pump Inhibitors (PPI). See our Gastroesophageal Reflux Disease Symptoms and Treatments page (coming soon) for more details.
Gastrointestinal leaks (including staple line leaks) occur when sealed or sutured (stitched) openings leak digestive contents into the abdomen. This can cause infection and abscess. Gastrointestinal leaks occur in as many as 5% of patients and can be repaired as long as it is caught early. Symptoms include fever, severe pain and a high heart rate. In order to prevent leaks, your surgeon should check the surgical connections a number of different ways, including 1) blowing air into the connection and observing whether any gets through and 2) using a dye to check for a leak. Leaks not discovered right away are usually treated by resting the stomach (being fed through an IV), but sometimes surgery is required to fix them.
General anesthesia complications – anesthesia risks increase withage and body mass index (BMI). Other health issues can also increase your risk, including circulatory or respiratory problems. However, anesthesia complications are usually minor and are relatively easy for your doctors to handle.
Hair loss – this can be an alarming side effect of rapid weight loss, but it is only temporary. It happens in about half of all patients in the year following surgery. Proper nutrition is the best defense, including protein and the right bariatric vitamins. Several other treatments can also help, including the application of special shampoos and oils (i.e. Nioxin shampoo, flax seed oil, biotin tablets or powder).
Heart attack (also called myocardial infarction) – an acute episode of heart disease marked by the death or damage of heart muscle due to insufficient blood supply, usually as a result of a coronary thrombosis or a coronary occlusion. Heart attacks are especially characterized by chest pain. The chances of having a heart attack during surgery are less than 0.5% (21).
Hemorrhage (bleeding) – a copious discharge of blood from the blood vessels. One study showed that out of 1,700 laparoscopic bariatric surgery patients only 3 had hemorrhagic complications, none of which needed to be converted to open operations or needed reoperations (22). However, other studies have shown internal bleeding to be as high as 4% following Roux-en-Y gastric bypass surgery. After the surgeon determines the type and severity of internal bleeding, it can be resolved in a number of ways: on its own, replenishing bodily fluids, stopping the use of all anticoagulation drugs and (rarely) by transfusion or reoperation (23).
Hernia – See Evisceration.
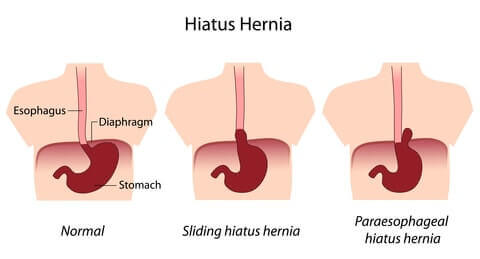
Hiatal Hernia – a hernia in which an anatomical part (such as the stomach) protrudes through the esophageal hiatus of the diaphragm. Hiatal hernias can occur after restrictive procedures when food causes the smaller stomach to bulge and push through the diaphragm. It is also not uncommon for an obese patient to already have a hiatal hernia before surgery. While it can be a “contraindication” for surgery(reason that you may not be able to have the surgery), hiatal hernias can also be repaired during bariatric surgery (24).
Hypoglycemia – Low blood sugar related to excessive insulin production. As a bariatric surgery complication, hypoglycemia is often the result of excessive dumping following Roux-en-Y gastric bypass surgery (25) (26). Medications can usually help mild to moderate conditions, however surgical removal of part or all of the pancreas (which produces insulin) may be required for more serious cases. Symptoms following surgery include rapid heart rate, shaking, sweating, confusion, feeling lightheaded, bad headaches or feeling overly hungry.
Incision(al) hernia – See Evisceration.
Indigestion – See Dyspepsia.
Infection – to contaminate with a disease-producing substance or agent (such as bacteria). Much more common in open surgeries than in laparoscopic surgeries due to the size of the external incisions. Usually treated with antibiotics.
Intolerance to certain foods – With a changed stomach size or digestive system, there will be certain foods that you’ll need to avoid and certain diet habits you’ll need to maintain. See our Bariatric Diet section for more. Also see Bowel Function Changes.
(none)
Kidney stones – stones in the kidney related to decreased urine volume or increased excretion of stone-forming components such as calcium, oxalate, urate, cystine, xanthine and phosphate. The stones form in the urine collecting area (the pelvis) of the kidney and may range in size from tiny to staghorn stones the size of the renal pelvis itself (27). Although additional research is needed, one study suggested that the risk of developing kidney stones increases after bariatric surgery due to changes in digestion and the resulting changes in the chemical makeup of patients’ urine. Click here to learn more.
Leaks – See Gastrointestinal Leak.
Malnutrition/Malabsorption – See Vitamin Deficiency.
Marginal Ulcers – Marginal ulcers are relatively common after Roux-en-Y gastric bypass, mini gastric bypass, and duodenal switch (Scopinaro procedure), and are the most common in the newly created stomach pouch after Roux-en-Y gastric bypass surgery.
Ulcers can usually be avoided by an appropriate bariatric diet , by not smoking and by staying away from NSAIDs (non-steroidal anti inflammatory drugs, including ibuprofen, Aleve, etc.). You can often tell if you have one because of a burning pain in the stomach. Your doctor can confirm ulcers with an endoscopy (a scope than is inserted through your mouth and down your esophagus) and usually treat them with antacids.
Nausea and vomiting are one of the most common side effects of bariatric surgery and are experienced in up to 70% of patients. In one study, patients reported feeling nauseous 1.4 times per week on average after gastric banding (lap band surgery) and 2.6 times per week after gastric bypass surgery (28). They also reported vomiting 0.9 times per week on average with the band and 0.2 times per week after gastric bypass. Following the doctor’s orders regarding your bariatric diet will typically fix or improve the problem. While in the hospital, receiving a larger amount of IV fluids at a faster rate may make you less likely to feel nauseous or vomit (29).
Organ injury during surgery – Caused by surgeon error during surgery. Injuries to your internal organs during surgery are a possibility, especially the bowel, stomach, spleen or esophagus due to their close proximity to the stomach/intestines.
Peritonitis – inflammation of the peritoneum (the smooth transparent serous membrane that lines the cavity of the abdomen, is folded inward over the abdominal and pelvic viscera, and consists of an outer layer closely adherent to the walls of the abdomen and an inner layer that folds to invest the viscera). Peritonitis after bariatric surgery is a serious complication that isusually caused by a gastrointestinal leak. Surgery is required to fixit (30).
Pneumonia – a disease of the lungs that is characterized especially by inflammation and consolidation of lung tissue followed by resolution. It is accompanied by fever, chills, cough, and difficulty breathing, and is caused chiefly by infection. Obese patients are more likely to develop pneumonia post-surgery, so it is important that patients begin deep breathing and coughing exercises following surgery to prevent it. These exercises are much easier after laparoscopic surgery than after open surgery. Should pneumonia develop, it can be treated with antibiotics.
Port problems occur in 20.5% or 1 in 5 gastric banding (lap band) patients (31).Port problems include…
- Port flip/inversion or dislodgement (10.3% of patients) – occurs when the lap band port (where fluids are taken out or added to the band) “flips over”. This is typically not a serious problem and a quick surgical procedure can turn it back over.
- Port Leak (1.1% – 4.9% of patients) – as with a band leak, patients can usually tell if their lap band system has a leak if their feelings of restriction decreases (i.e. the amount they can eat increases) over time without the doctor unfilling the port. To determine if you have a port leak, your doctor may inject colored fluid and take an X-Ray to see if any of the colored fluid is present (from a leak) outside of the lap band system. Surgery is usually required to repair it.
- Port or band infection (1.5% – 5.3% of patients) – if port or band infection occurs, it is usually healed with antibiotics, but removal of the band or port may be necessary.
- Port dislocation (6.9% of patients) – similar to a port flip, a port dislocation means that your port has moved from its original location. It can be fixed with a simple operation under local anesthesia.
Postoperative bleeding – refers to internal bleeding following bariatric surgery.See Hemmorhage.
Pouch dilation – refers to the enlarging of the pouch created after certain types of surgery. For lap band surgery patients, it may be fixed by removing fluid from the band. For all procedures with a pouch, surgery is sometimes required to tighten it (32).
Pulmonary embolism – embolism (the sudden obstruction of a blood vessel by an abnormal particle, such as a bubble, circulating in the blood) of a pulmonary artery or one of its branches that is produced by foreign matter (most often a blood clot originating in a vein of the leg or pelvis) that is marked by labored breathing, chest pain, fainting, rapid heart rate, cyanosis, shock, and sometimes death. Also see Blood Clots and Deep Vein Thrombosis.
(none)
Respiratory failure is a rare but serious complication (33).It occurs when oxygen and carbon dioxide levels fall too far outside of their normal ranges. Hospital treatment includes drugs and ventilation, among other techniques.
Sepsis – See Wound Sepsis.
Skin Changes such as acne or dry skin occur with some patients. The right bariatric diet and bariatric vitamins are your best defense. There are also many over the counter creams and lotions that can help. Worst case, partner with your dermatologist to find a treatment that works.
Spleen damage – See Organ Injury During Surgery.
Staple line leak – See Gastrointestinal Leak.
Stoma obstruction – a partial or complete blockage of the new or altered digestive opening created during bariatric surgery. See Food Trapping.
Stenosis/Stricture – a narrowing or constriction of the diameter of a bodily passage or orifice. This is most common in procedures that rearrange your digestive system such as gastric bypass surgery (up to 8% of patients) and duodenal switch surgery and results from a build-up of scar tissue between your intestine and your reduced stomach or at an intestine-to-intestine connection (anastomosis).
The primary symptom is almost always vomiting, and it is usually treated by inserting and inflating a balloon to stretch the connection between the stomach and intestine. GERD and older age increase the risk of strictures (34).
Stroke– sudden diminution or loss of consciousness, sensation and voluntary motion caused by rupture or obstruction (as by a blood clot )of a blood vessel of the brain. Obese patients have a higher general risk of stroke, and bariatric surgery has been shown to reduce the risk (35).
Thrombus – See Blood Clots
Thrombophlebitis – inflammation of a vein with formation of a thrombus (a clot of blood formed within a blood vessel and remaining attached to its place of origin). The body’s response could be to produce more clots which increase the risk of Deep Vein Thrombosis and Pulmonary Embolism. Also see Blood Clots.
Tired feeling – See Body Feeling Changes.
Thrush (yeast infection) – this can be a side effect of the antibiotics you are on to prevent infection immediately following surgery. Symptoms include changes to your tongue such as a white coating, redness or inflammation. This is easily cured with medicine, so let your doctor know if this starts to develop.
Ulcers – See Marginal Ulcers.
Vitamin and mineral deficiency / malnutrition / malabsorption – symptoms include fatigue, anemia, and osteoporosis and are usually completely avoided by strictly following your doctor’s prescribed vitamin and supplement regimen. You should also have blood work at least semi-annually to make sure that you continue to receive the proper amounts. (See our Bariatric Vitamins page for the problems associated with vitamin deficiency)
Vomiting –See Nausea and Vomiting.
Weak feeling – See Body Feeling Changes.
Weight regain – Most bariatric surgery patients will experience some weight regain after the lowest weight level is reached. See our Weight Gain after Bariatric Surgery page for more.
Wound infection – See Infection.
Wound reopening refers to the opening of the external incisions made during bariatric surgery. It is much more likely to occur following an open procedure than with a laparoscopic procedure.
Wound sepsis (and sepsis in general) – a systemic response typically to a serious localized infection (as of the abdomen or lungs) especially of bacterial origin that is usually marked by abnormal body temperature and white blood cell count, tachycardia and tachypnea; specifically: a systemic inflammatory response syndrome induced by a documented infection.
While wound sepsis can occur from any source of infection, this serious complication often results from a gastric fistula. Due to the risk of wound sepsis following a gastric fistula, the fistula must be treated immediately and effectively in order to avoid sepsis (36). If sepsis does develop, patients are often treated in the intensive care unit with IV fluids and antibiotics.
Yeast infection – See Thrush.

