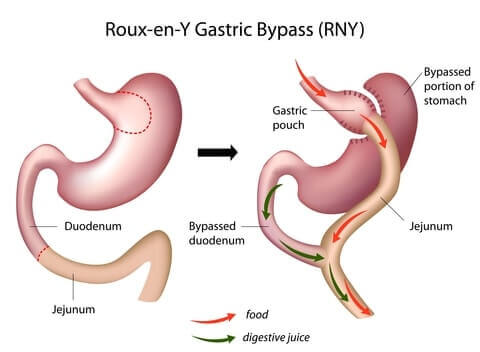
Gastric bypass surgery (“Roux-en-Y gastric bypass”) makes the stomach smaller and reroutes the intestines. As a result, patients:
- Feel full sooner after eating
- Absorb less food
- Lose up to two-thirds of their excess weight within 2 years
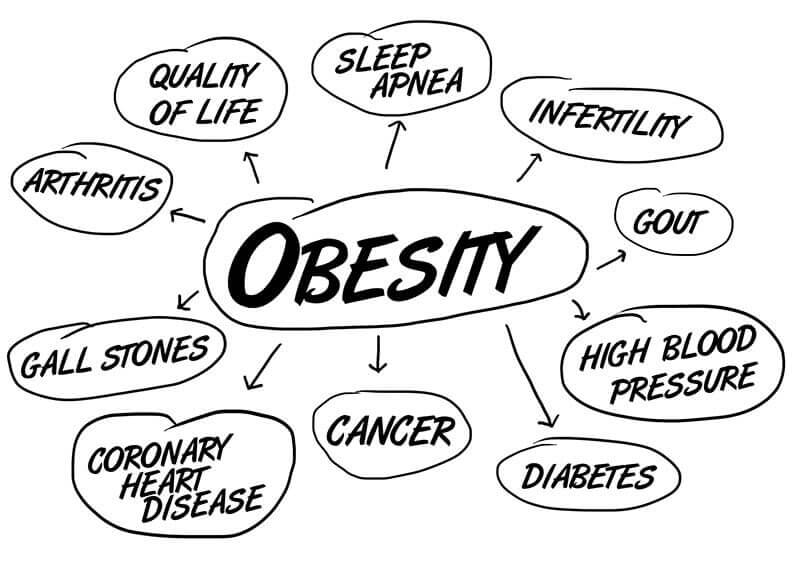
- Have significant health improvement
This page covers everything you need to determine whether gastric bypass is the right weight loss procedure for you.

Weight Loss
Half to Most of Your Excess Weight 
Weight Loss – Half to Most of Your Excess Weight
Gastric bypass patients usually lose a lot of weight very quickly. Within 3 months, the average patient will lose about one-third of their excess weight. By the one-year mark, almost two-thirds of the excess weight will be gone.
Many patients reach “peak” weight loss between one and two years, then gain a little back (more about Weight Regain in the “Downsides” section below). But long-term results are still impressive, with the average patient keeping about 60% of their excess weight off.
Keep in mind that these are averages – “middle of the road” results. Patients who eat the right foods, exercise regularly, and follow their surgeon’s advice can lose even more, while patients who veer off-track lose less.
Cost
$24,000 Avg Before Discounts, $2,000 Avg With Insurance
Cost – $24,000 Avg Before Discounts, $2,000 Avg With Insurance
On average, the all-in cost of gastric bypass equals (in U.S. Dollars for comparison purposes):
- United States – $24,000 (ranges from $15,000 in Arkansas to $57,000 in Alaska)
- Canada – $20,000
- Australia – $17,000
- Mexico – $7,400
- India – $10,400
- Thailand – $10,500
- Costa Rica – $12,500
However, your out-of-pocket costs depend on several factors including:
- Whether your procedure is open or laparoscopic – open gastric bypass surgery tends to cost about $2,500 more than laparoscopic surgery, on average (33)
- Which hospital you have the surgery in
- Whether or not you have insurance – if your surgeon and hospital are covered by your insurance, it is likely that a discount has been negotiated to allow that surgeon and hospital to participate in your insurance company’s network
- Whether you obtain financing for some or all of the costs
- Specific fees your bariatric surgeon and other professionals charge for the various pre-op, surgical, and post-op services.
Note that the above averages include total costs incurred during surgery. Some surgeons also include Pre-Op costs in their quoted fees (more on Pre-Op and Post-Op fees below).
However, the above averages do not include Post-Op costs which will be based on your specific circumstances.
Total surgery costs can be further complicated by:
- Self-Pay Discounts – Most weight loss surgery clinics will offer some sort of self-pay discount or payment plan if you don’t have insurance (or if insurance won’t cover the procedure). All you have to do is ask!
- Other Discounts – Additional discounts may be offered for things like full up-front payment. Ask your surgeon’s office if there are any other discounts that you might be able to take advantage of.
- Same Surgeon, Different Hospitals – Some surgeons have “operating privileges” at more than one hospital. Since hospital costs can vary widely – even in the same town and regardless of quality – ask your surgeon if you have a choice.
Gastric bypass fees are split between Pre-Op, Surgery, and Post-Op services:

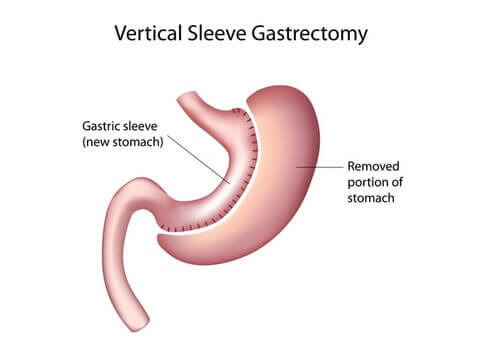
Procedure
Laparoscopic, Creates Small Stomach Pouch, & Reroutes Small Intestine
Procedure – Laparoscopic, Creates Small Stomach Pouch, & Reroutes Small Intestine
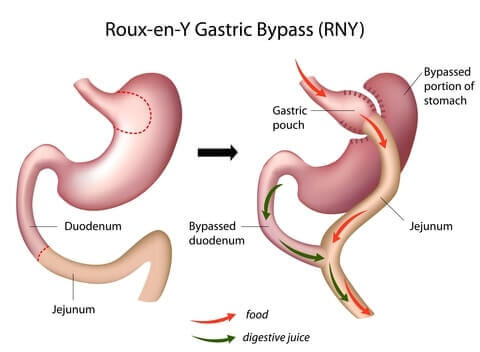
Why Gastric Bypass Works
- Reduced stomach size makes the patient feel full sooner after eating
- Rearranged intestines causes the body to absorb fewer minerals
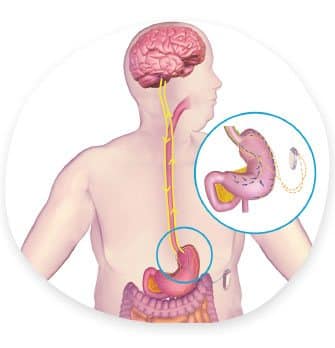
- Dumping syndrome symptoms deter patients from eating unhealthy foods
Recovery
2 – 3 Days in Hospital, Back to Work in 2 Weeks, 4 – 6 Weeks to Full Recovery

Diet & Life After – Restricted Diet, Less Hungry, Full Sooner, Lifelong Supplements, Regular Exercise, Changing Relationships
Gastric bypass leads to impressive weight loss and health improvement, but what will day-to-day life be like? What are the tradeoffs?
Your surgery is only a tool, and long-term success requires diligence and sometimes difficult change in other areas.
Following is what to expect…
Exercise: 2.5 hours per week, spread out over 2 to 4 days

Exercise is almost as important as what you eat after gastric bypass surgery for two big reasons:
- Patients who exercise regularly lose more weight over the long-term
- Physical and mental health benefits make you much more likely to keep your new lifestyle requirements in line
How much exercise do you need to for noticeable results?
One study found that exercising 2.5 hours per week leads to 5.7% more weight loss (50). Another showed that gastric bypass patients who exercise at least 30 minutes a day, 3 days per week have a 4+% lower body mass index (51).
Further, regular exercise leads to quicker improvement in obesity-related health problems following surgery (52).
To help you stay on track:
- Block out time to exercise at the same times on the same days of the week.
- Spread your workouts over 3 or 4 days each week rather than having one or two long sessions. In addition to building endurance, this will make working out less intimidating.
Your Brain: Less Hungry, Careful About Food Addiction, New Mentality Will Change Behavior & Relationships
Relationships After Weight Loss

Gastric bypass leads to rapid and significant weight loss, and people will start treating you differently within a couple of months after surgery. Following are positive experiences reported by most patients:
- Treated with more respect
- More romantic interest from others
- No more obesity discrimination
- Deeper relationships as a result of being able to physically keep up with kids and more physically fit friends
- More compliments from others
- Increased self-confidence
However, being “newly thin” may carry unforeseen negatives as well:
- How will overweight friends or family members feel when you’re losing weight but they are not?
- If they’re not making diet and lifestyle changes as well, will your friends or family make it more difficult for you to stay on track?
- How will your coworkers react? Should you even tell them you are having surgery?
- Will your new healthier diet and smaller portion sizes make meals with others awkward?
- Could intimacy with your spouse or partner be effected?
- Could your spouse or partner become jealous now that others are noticing you more?
The way you view people and relationships may change as well. Common thoughts include:
- “Would this person be treating me the same way if I hadn’t lost all of this weight?”
- “How do I handle obesity discrimination now that I’m on the “other side”?”
For real life experiences and advice from other gastric bypass patients, see our Relationships After Weight Loss surgery page.
Downsides
Risk of Complications, Side Effects, & Weight Regain
Downsides – Risk of Complications, Side Effects, & Weight Regain

Like all bariatric surgery procedures, mortality rates for gastric bypass (risk of dying) are extremely low. It has a survival rate of 998 out of every 1,000 patients.
However, complications are more common, with about to 1 out of 7 patients experiencing one or more over the long-term (53, 54).
Vs Other Types of Surgery – Similar or Better Weight Loss & Health Improvement, Similar or Higher Risk of Complications & Side Effects

Gastric bypass was considered the “gold standard” procedure for several years, until gastric sleeve surgery took its place.
However, it is still recommended by surgeons for some patients for its unique combination of benefits.
Picture of Procedure (click to expand) Picture of Procedure (click to expand) |
Video of Procedure Video of Procedure |
External Device Placed Inside Body? External Device Placed Inside Body? |
Year Device/Product Approved Year Device/ Product Approved |
Average Total Cost Before Insurance (U.S.) Average Total Cost Before Insurance (U.S.) |
Covered by Insurance? Covered by Insurance? |
Financing Available? Financing Available? |
BMI Requirements BMI Requirements |
Avg % Excess Weight Loss After 5 Years Avg % Excess Weight Loss After 5 Years |
Health Improvement Health Improvement |
Procedure Type Procedure Type |
Complication Rate Complication Rate |
Mortality Rate Mortality Rate |
Reversible? Reversible? |
Time Until Removed Time Until Removed |
Alters Path of Digestion (Higher Risk of Mal-absorption)? Alters Path of Digestion (Higher Risk of Mal-absorption)? |
Procedure Time (Average) Procedure Time (Average) |
Hospital Stay (Average) Hospital Stay (Average) |
Recovery Time (Back to Work) – Average Recovery Time (Back to Work) – Average |
Diet Challenges (Procedure-Specific; Click here for general diet changes to expect) Diet Challenges (Procedure-Specific; Click here for general diet changes to expect) |
Food Cravings Likely to Decrease? Food Cravings Likely to Decrease? |
Difficulty Swallowing? (due to food backing up because of smaller stomach) Difficulty Swallowing? (due to food backing up because of smaller stomach) |
Digestion & Bowel Movement Post-Recovery (Relatively common issues) Digestion & Bowel Movement Post-Recovery (Relatively common issues) |
Qualified Surgeons Qualified Surgeons |
Patient Guides Patient Guides |
Gastric Bypass |
Picture of Procedure (click to expand) |
External Device Placed Inside Body? No |
Year Device/Product Approved n/a |
Average Total Cost Before Insurance (U.S.) $24,000 |
Covered by Insurance? Yes (other than some individual policies) |
Financing Available? Yes |
BMI Requirements 35 – 39.9 with health problems; 40+ without |
Avg % Excess Weight Loss After 5 Years 50 – 70% |
Health Improvement Compare % excess weight loss; the more weight loss, the more health improvement
|
Procedure Type Laparoscopic |
Complication Rate Up to 15% |
Mortality Rate 0.24% |
Reversible? No |
Time Until Removed n/a |
Alters Path of Digestion (Higher Risk of Malabsorption)? Yes |
Procedure Time (Average) ~4 hours |
Hospital Stay (Average) 2 to 3 days |
Recovery Time (Back to Work) – Average ~2 weeks |
Diet Challenges (Procedure-Specific; Click here for general diet changes to expect) Potential problem foods:Sugars, Refined fats, Carbs, Dairy. Malabsorption will require life-long vitamin supple-mentation. |
Food Cravings Likely to Decrease? Maybe |
Difficulty Swallowing? (due to food backing up because of smaller stomach) Possible |
Digestion & Bowel Movement Post-Recovery (Relatively common issues) Dumping syndrome occurs in ~80% of patients who eat sugar, refined fats, or carbs. |
Qualified Surgeons Broad Network – Click Here to Find Surgeon |
Patient Guides (this page) |
Gastric Sleeve |
Picture of Procedure (click to expand) |
External Device Placed Inside Body? No |
Year Device/Product Approved n/a |
Average Total Cost Before Insurance (U.S.) $19,000 |
Covered by Insurance? Yes (other than some individual policies) |
Financing Available? Yes |
BMI Requirements 35 – 39.9 with health problems; 40+ without |
Avg % Excess Weight Loss After 5 Years 64 – 75% |
Health Improvement Compare % excess weight loss; the more weight loss, the more health improvement |
Procedure Type Laparoscopic |
Complication Rate Up to 10% |
Mortality Rate 0.19% |
Reversible? No |
Time Until Removed n/a |
Alters Path of Digestion (Higher Risk of Malabsorption)? No |
Procedure Time (Average) ~2 hours |
Hospital Stay (Average) 2 to 3 days |
Recovery Time (Back to Work) – Average ~2 weeks |
Diet Challenges (Procedure-Specific; Click here for general diet changes to expect) Potential problem foods: Dairy |
Food Cravings Likely to Decrease? Maybe |
Difficulty Swallowing? (due to food backing up because of smaller stomach) Possible |
Digestion & Bowel Movement Post-Recovery (Relatively common issues) GERD (reflux) in ~1 out of 5 patients after 1 year, drops to 1~ out of 33 patients after 3 year.
Some patients experience diarrhea. |
Qualified Surgeons Broad Network – Click Here to Find Surgeon |
Patient Guides |
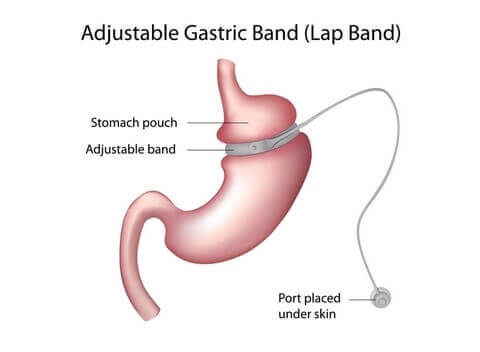
Lap Band |
Picture of Procedure (click to expand) |
External Device Placed Inside Body? Yes |
Year Device/Product Approved 2011 (FDA10) |
Average Total Cost Before Insurance (U.S.) $15,000 |
Covered by Insurance? Yes (other than some individual policies) |
Financing Available? Yes |
BMI Requirements 35 – 39.9 with health problems; 40+ without |
Avg % Excess Weight Loss After 5 Years 25 – 80% (extremely variable among patients) |
Health Improvement Compare % excess weight loss; the more weight loss, the more health improvement |
Procedure Type Laparoscopic |
Complication Rate Up to 33% |
Mortality Rate 0.10% |
Reversible? Yes |
Time Until Removed Patient-Specific (not necessarily required) |
Alters Path of Digestion (Higher Risk of Malabsorption)? No |
Procedure Time (Average) ~1 hour |
Hospital Stay (Average) Outpatient to 1 day |
Recovery Time (Back to Work) – Average ~2 weeks |
Diet Challenges
(Procedure-Specific; Click here for general diet changes to expect) Potential problem foods: Dairy.
Should not drink anything within 30 minutes before or after eating |
Food Cravings Likely to Decrease? No |
Difficulty Swallowing? (due to food backing up because of smaller stomach) Possible |
Digestion & Bowel Movement Post-Recovery (Relatively common issues) Reflux and vomiting common if band too tight (can be adjusted).
Some patients experience constipation. |
Qualified Surgeons Broad Network – Click Here to Find Surgeon |
Patient Guides |
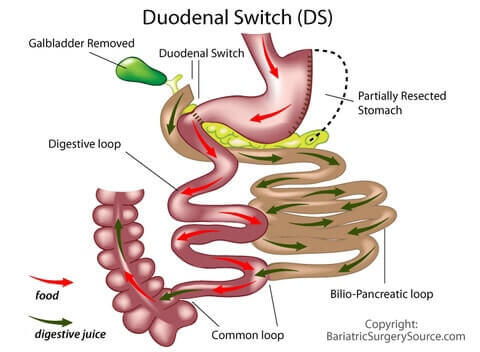
Duodenal Switch |
Picture of Procedure (click to expand) |
External Device Placed Inside Body? No |
Year Device/Product Approved n/a |
Average Total Cost Before Insurance (U.S.) $27,000 |
Covered by Insurance? Yes (other than some individual policies) |
Financing Available? Yes |
BMI Requirements 35 – 39.9 with health problems; 40+ without
(but more common for 50+) |
Avg % Excess Weight Loss After 5 Years 65 – 75% |
Health Improvement Compare % excess weight loss; the more weight loss, the more health improvement |
Procedure Type Laparoscopic |
Complication Rate Up to 24% |
Mortality Rate Up to 1.1% (but procedure tends to be performed on heavier patients who have higher risk) |
Reversible? No |
Time Until Removed n/a |
Alters Path of Digestion (Higher Risk of Malabsorption)? Yes |
Procedure Time (Average) 3.5 – 4.5 hours |
Hospital Stay (Average) 2 to 3 days |
Recovery Time (Back to Work) – Average ~2 weeks |
Diet Challenges(Procedure-Specific; Click here for general diet changes to expect) Malabsorption will require life-long vitamin supple-mentation. |
Food Cravings Likely to Decrease? Maybe |
Difficulty Swallowing? (due to food backing up because of smaller stomach) Possible |
Digestion & Bowel Movement Post-Recovery (Relatively common issues) Might be significant, including frequency, diarrhea, and/or foul-smelling stools/ flatulence. |
Qualified Surgeons Fewer Options – Click Here to Find Surgeon |
Patient Guides |
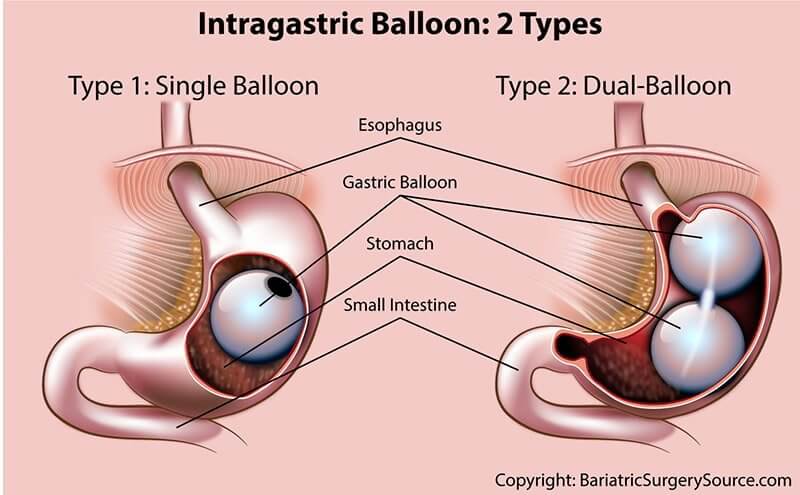
Gastric Balloon |
Picture of Procedure (click to expand) |
External Device Placed Inside Body? Yes |
Year Device/Product Approved 2015 (FDA11) |
Average Total Cost Before Insurance (U.S.) $8,150 |
Covered by Insurance? Possible with aggressive negotiation and appeals |
Financing Available? Yes |
BMI Requirements Between 30 & 40 in U.S. (above 27 elsewhere) |
Avg % Excess Weight Loss After 5 Years n/a (must be removed after 6 months; weight loss during that time is 26 – 46%) |
Health Improvement Compare % excess weight loss; the more weight loss, the more health improvement |
Procedure Type Through Mouth |
Complication Rate Up to 10% |
Mortality Rate Close to 0% |
Reversible? Yes |
Time Until Removed 6 months max |
Alters Path of Digestion (Higher Risk of Malabsorption)? No |
Procedure Time (Average) 30 minutes or less |
Hospital Stay (Average) Outpatient |
Recovery Time (Back to Work) – Average 3 – 4 days |
Click here for general diet changes to expect) Potential Problem Foods: Pasta and other foods that might stick to balloon in stomach. |
Food Cravings Likely to Decrease? No |
Difficulty Swallowing? (due to food backing up because of smaller stomach) Unlikely |
Digestion & Bowel Movement Post-Recovery (Relatively common issues) Vomiting possible (but often avoidable with proper habits). “Feeling bloated” reported by some patients. |
Qualified Surgeons Fewer Options – Click Here to Find Surgeon |
Patient Guides |
vBloc |
Picture of Procedure (click to expand) |
External Device Placed Inside Body? Yes |
Year Device/Product Approved 2015 (FDA9) |
Average Total Cost Before Insurance (U.S.) $18,500 |
Covered by Insurance? Possible with aggressive negotiation and appeals |
Financing Available? Yes |
BMI Requirements 35 – 39.9 with health problems; 40 – 45 without (none over 45) |
Avg % Excess Weight Loss After 5 Years 17 – 28% |
Health Improvement Compare % excess weight loss; the more weight loss, the more health improvement |
Procedure Type Laparoscopic |
Complication Rate 3 – 4% |
Mortality Rate Close to 0% |
Reversible? Yes |
Time Until Removed Patient-Specific (not necessarily required) |
Alters Path of Digestion (Higher Risk of Malabsorption)? No |
Procedure Time (Average) 60 to 90 minutes |
Hospital Stay (Average) Outpatient |
Recovery Time (Back to Work) – Average 3 – 4 days |
Diet Challenges (Procedure-Specific; Click here for general diet changes to expect) None, but healthier eating recommended for better results |
Food Cravings Likely to Decrease? Yes |
Difficulty Swallowing? (due to food backing up because of smaller stomach) No |
Digestion & Bowel Movement Post-Recovery (Relatively common issues) None |
Qualified Surgeons Fewer Options – Click Here to Find Surgeon |
Patient Guides |
Find a Gastric Bypass Surgeon
DISCLAIMER : Information received via BariGroups group meetings or during coaching sessions should NOT be relied upon for personal, legal or medical decisions and you should consult with your doctor or other licensed professional before beginning and during any course of medical treatment. By using BariGroups, you are confirming that you agree with our Terms & Conditions (click here to review).
I agree